
5 Tips to keep the shoulders (and neck) healthy
By: Mark Z. Jamantoc, PT, OCS, FDM-IC, PPSC
About the AuthorHere are some quick ways to keep your shoulder healthy and prevent (or improve) discomforts caused by possible impingement issues. Patients are always asking me for specific stretches to improve neck and shoulder. Here are some great ways to do them. As always, this article will not replace medical advice coming from your doctor or your physical therapist. This was written for educational purpose only.

1. Stretch the Pecs. The chest muscles are mainly composed of pectorals: Pectoralis major and Pectoralis minor. I wanted to give special attention to the Pec minor since it has attachments to the 3rd, 4th, 5th ribs and the coracoid process of the scapula. Thus, when the pectoralis minor is tight, it causes a multitude of issues for the shoulder (and sometimes the front of the neck area as well).
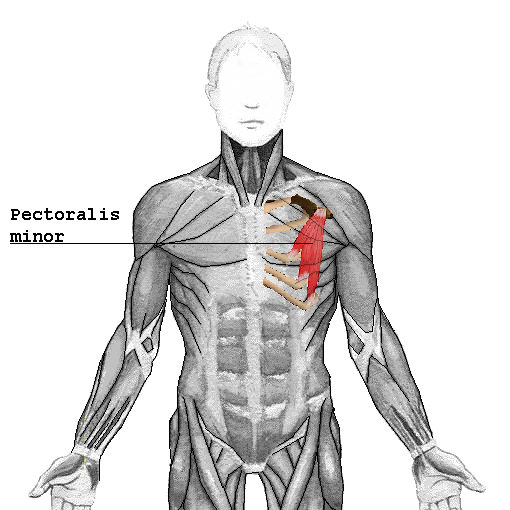
Pectoralis major and minor stretch by Brent Brookbush:
2. Stretch your neck and top of the shoulders. As the neck is connected to the shoulders, when I evaluate the neck, I never ignore the shoulders. The key muscles are the scalenes and the upper trapezius, both of which have huge influences on the top ribs: 1 and 2. When these muscles are tight, they can pull the 1st and 2nd ribs out and cause some major issues in the neck and the shoulder and may cause some symptoms resembling thoracic outlet syndrome. A study showed that a subluxed 2nd rib can actually resemble an impinged shoulder. It is important to stretch a major muscles that surround this region.
Here are a few quick stretches that you can start incorporating daily:
Scalenes:
Alternative chest stretch
Levator scapula stretch
Posterior shoulder stretch
Upper trapezius stretch
Triceps stretch
STRETCH THE LEVATOR SCAPULAE. I see so many shoulder patients that have tight levator scapulae muscles, hence I am giving this muscle a bit more attention here. More often than not, I would find the C1 to C4 on that side hypomobile because of the pull of this muscle and therefore, can cause some major neck pain or symptoms. After all, it is attached to the transverse processes of the first four cervical vertebrae.

Here is a great video by my friend Brent Brookbush, DPT, MS, PES, CES, CSCS, ACSM-H/FS, owner and president of Brent Brookbush Institute of Movement Science on a dynamic stretch for the levator scapulae muscle. This is actually one of my own personal favorites.
3. DON'T FORGET THE ARMS. That would be your Biceps brachii and Triceps brachii muscles. Studies have shown that working on these antagonistic muscles while you're strengthening your rotator cuff WILL help with shoulder strength and ultimately, scapular stability. I was one of those who were guilty enough in the past to not give these muscles a workout routine as a patient's homework.


In a pubmed study, the conclusions state: Supraspinatus activity is similar between 'empty can' and 'full can' exercises, although the 'full can' results in less risk of subacromial impingement. Infraspinatus and subscapularis activity have generally been reported to be higher in the 'full can' compared with the 'empty can', while posterior deltoid activity has been reported to be higher in the 'empty can' than the 'full can'.
RELATED READING: YOUR NECK PAIN COULD BE A LATS PROBLEM


Comments
Post a Comment